

Changes in total and differential leukocyte counts are usually grouped into patterns that facilitate interpretation.
These patterns are:
- Stress leukogram
- Physiologic leukocytosis
- Inflammatory leukogram
- Leukemoid reaction
Evaluating common white blood cell inflammatory patterns
Eric Isselée / stock.adobe.com

Content sponsored by Zoetis
These patterns are:
Cortisol release by the adrenal gland will occur as a result of a wide range of processes, including systemic illness, metabolic disturbances, pain, etc., and will be mimicked by corticosteroid therapy.
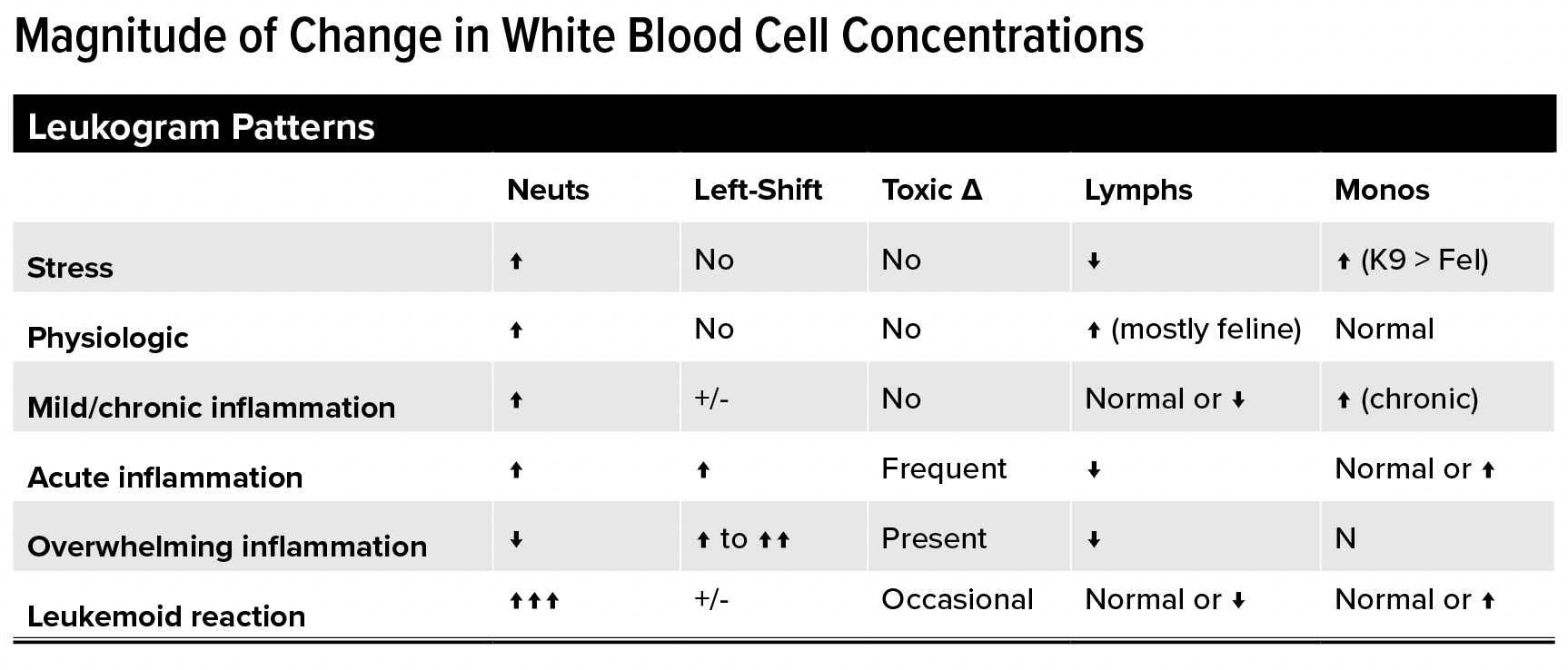
Pattern: The classic stress leukogram pattern includes neutrophilia, lymphopenia, monocytosis, and eosinopenia.
Not all of these changes will be present in every patient. The most consistent finding is mild mature neutrophilia (generally with no left shift), followed by lymphopenia. Monocytosis from corticosteroids is common in dogs, but can be uncommon in cats.
This leukogram pattern is due to epinephrine or norepinephrine release. It is also called a “flight or fight” response. This pattern is most commonly seen in cats (of any age), and possibly in younger animals of other species. These changes are usually transient and will generally resolve about 30 minutes after the patient relaxes.
Pattern: The classic physiological leukocytosis pattern is mild neutrophilia (mature cells with no left shift) and lymphocytosis, sometimes called a “physiologic lymphocytosis.”

The inflammatory leukogram pattern depends on the timing of sample collection and represents the balance between tissue consumption and bone marrow production. The neutrophil numbers in inflammation can vary from severely depressed to markedly increased. A left shift indicates the presence of immature neutrophils in blood and usually, but not always, indicates an inflammatory leukogram.
This leukogram pattern can be variable depending on the source and severity of the inflammation. The changes discussed below are often identified on the complete blood cell count from patients with inflammation, but it is possible to have inflammation in an animal that does not show an inflammatory leukogram.
Tissue demand is met or exceeded by increased marrow production and release of both segmented and immature neutrophils.
Pattern: Variable neutrophilia with varying degrees of left shift and toxic changes.
Tissue demand and marrow production are balanced. Release of immature neutrophils may not be required to meet demand.
Pattern: Neutrophils numbers may be normal or marginally increased. Left shift is only mild or absent because the bone marrow adequately supplies the demand. Toxic changes generally are not observed.
Tissue demand surpasses the ability of the marrow to deliver inflammatory cells to the blood. There are few cells in the circulating pool. Those present will usually be immature.
Pattern: Normal or decreased number of neutrophils with a left shift, which may include more immature forms than bands (metamyelocytes, myelocytes). Some patients may have more immature than mature/segmented neutrophils (degenerative lef shift). Moderate to severe toxic change in neutrophils should be present.
Monocytosis: This may be part of an inflammatory leukogram. It is usually observed with more long-standing or resolving inflammation. However, in some patients, the increase in monocytes is quite mild.
Lymphopenia (with or without eosinopenia): Frequently accompanies an inflammatory leukogram but does not always happen. This is usually attributed to concurrent endogenous stress (corticosteroid release). In some cases, a mild lymphocytosis may be seen with chronic inflammatory conditions that incite a decent antigenic response. Causes of inflammation are many and include:
Pattern: This leukogram is characterized by a marked neutrophilic leukocytosis (>50,000 cells/μL) with a concurrent, orderly left shift. Toxic changes may or may not be present.
It is called “leukemoid reaction” because it resembles granulocytic leukemia but is caused by some other process. It is also referred to as extreme neutrophilic (granulocytic) leukocytosis.
Both stress and inflammation can manifest with relatively similar leukogram patterns (eg, mature neutrophilia, monocytosis, lymphopenia, and eosinopenia), although all changes may not be present in every patient. Under these conditions, it is unclear from a single hemogram whether the changes are due to stress or inflammation. In these cases, other clinical data (eg, fever) and laboratory data (eg, hyperglobulinemia, hypoalbuminemia, hypoferremia) should be used to determine the more likely cause. Knowing the degree of change may also be helpful because a stress leukogram is uncommon in species other than dogs and is usually associated with a mild increase in neutrophils.
Remember that a single hemogram is a snapshot in time. Hemogram changes can occur quite rapidly. Therefore, monitoring hemogram results frequently (every 12-24 hours) can be very helpful in determining the course of an inflammatory response and response to treatment. Never treat laboratory data, always treat the patient.





